| There are several time honored procedures
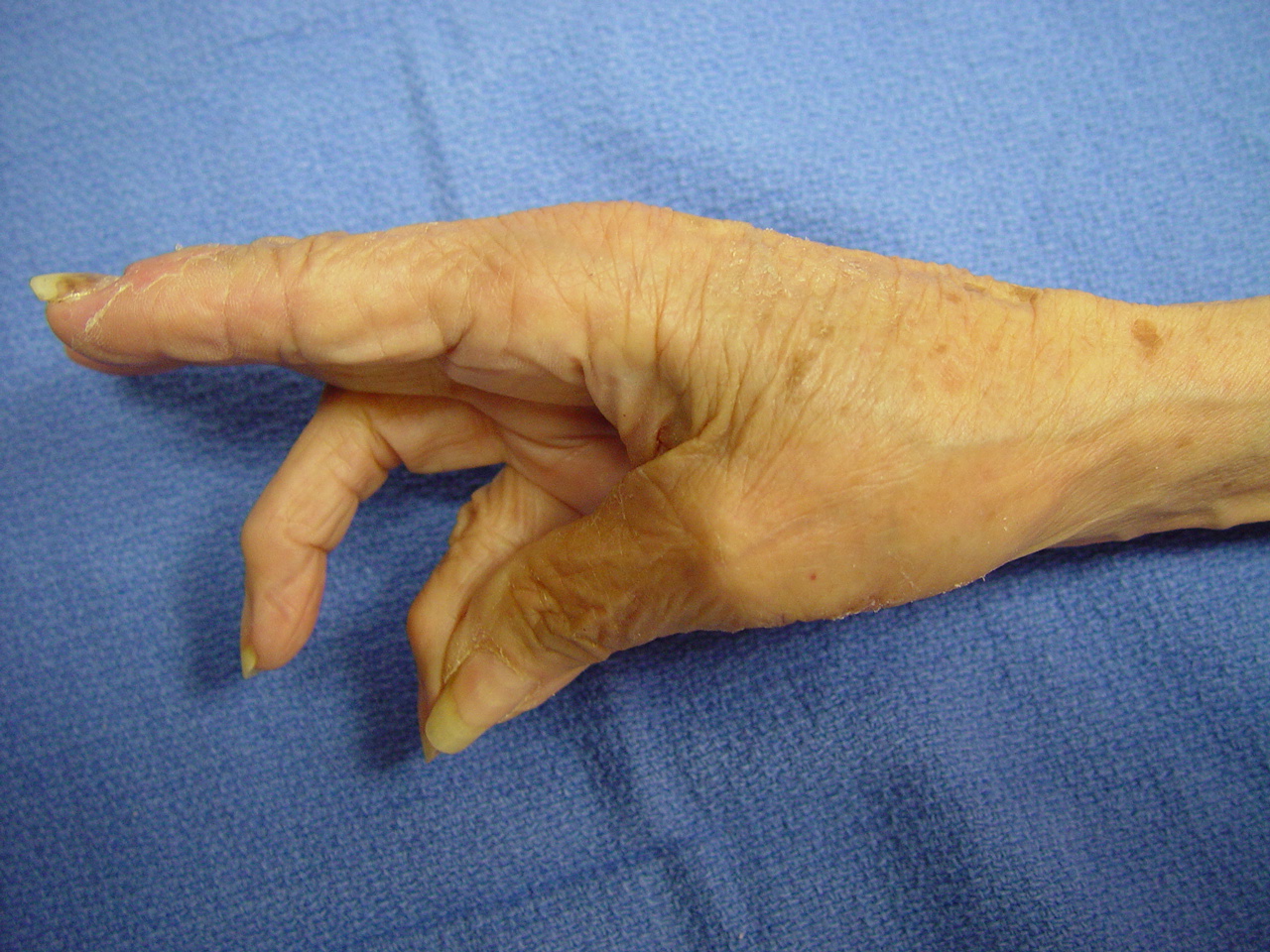
for restoration of thumb abduction in median nerve palsy, including transfer
of the palmaris longus, superficial flexor, extensor indicis, extensor
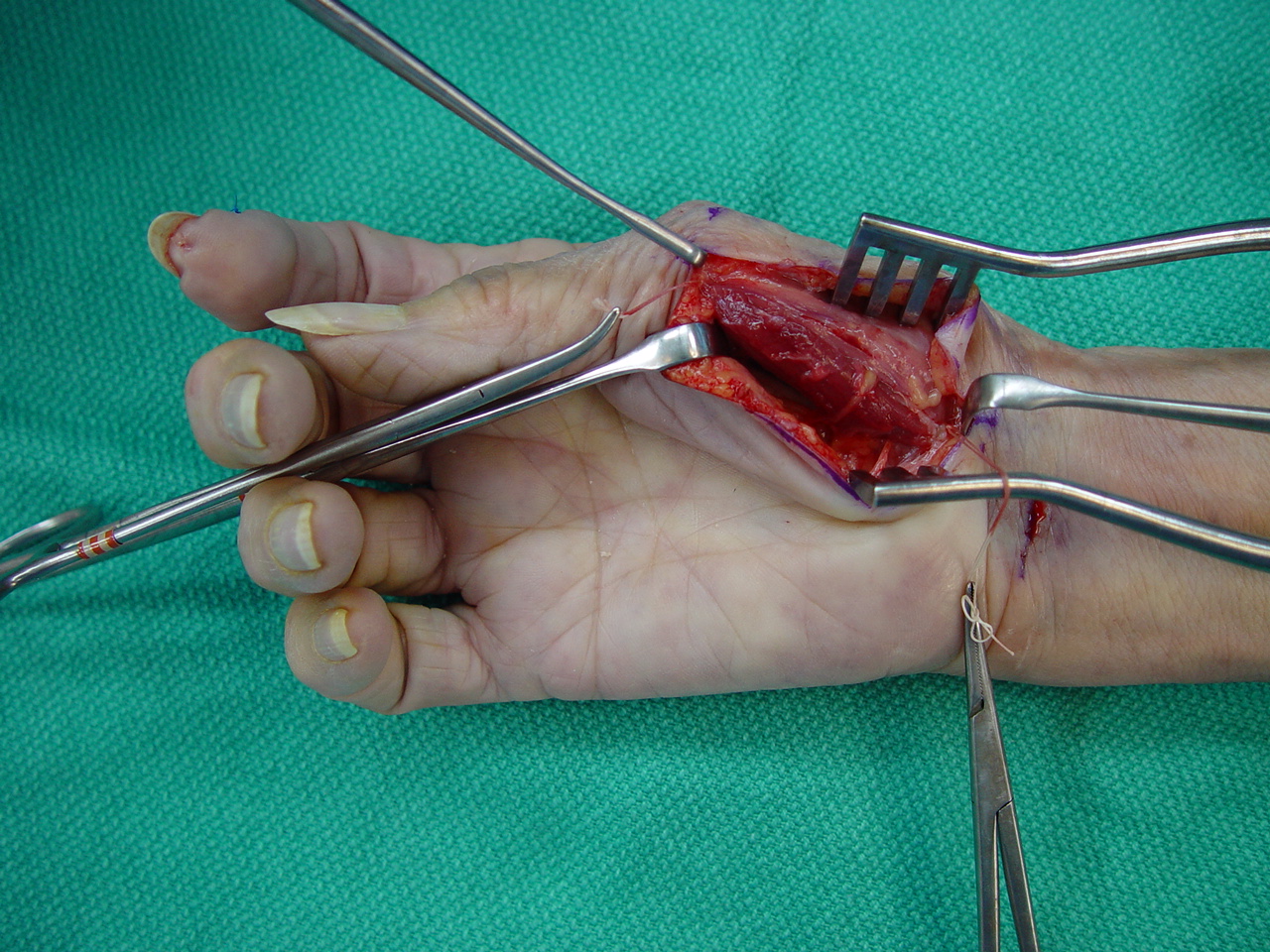
digiti minimi, and others. This is a description of a new procedure, a
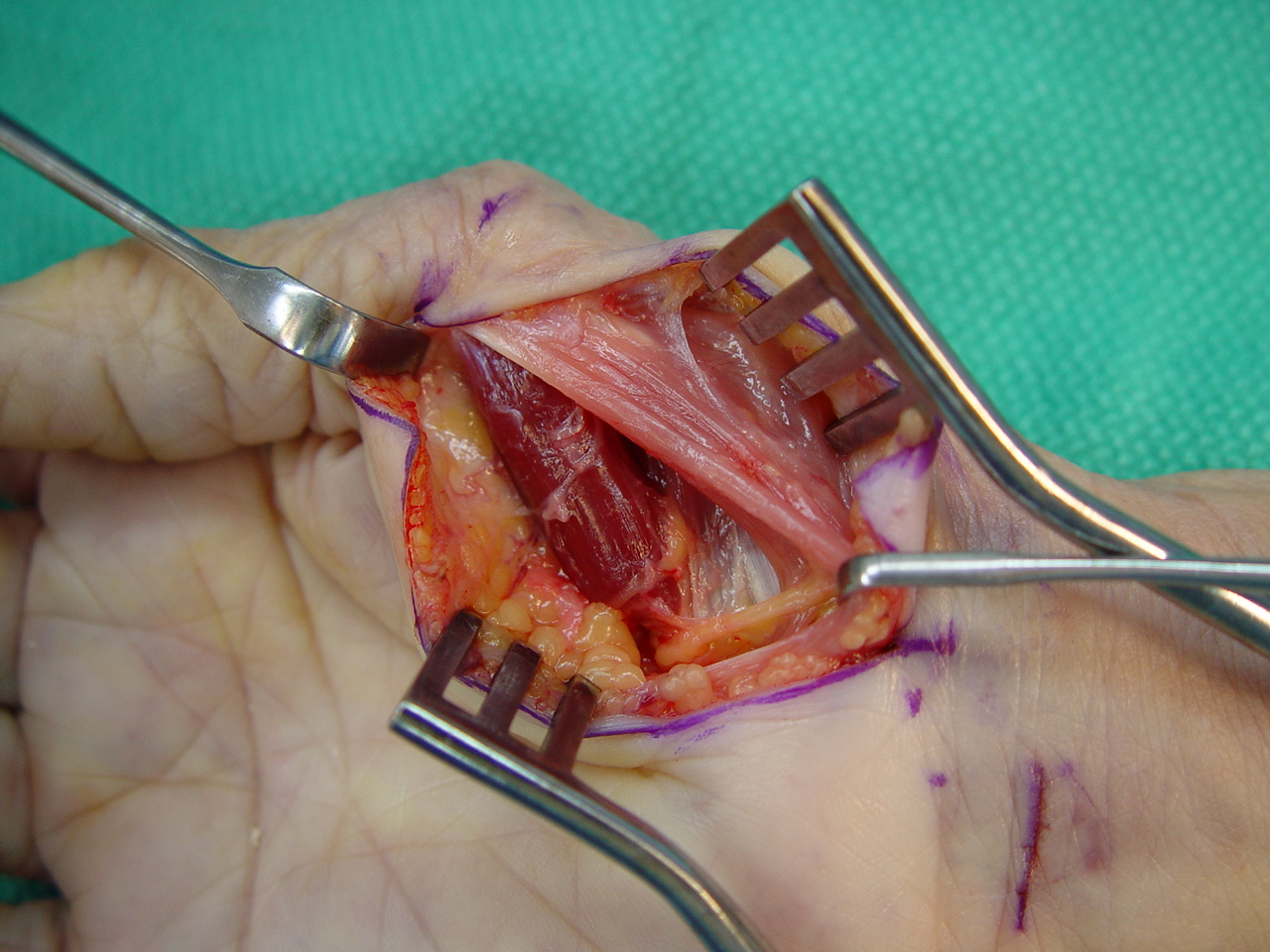
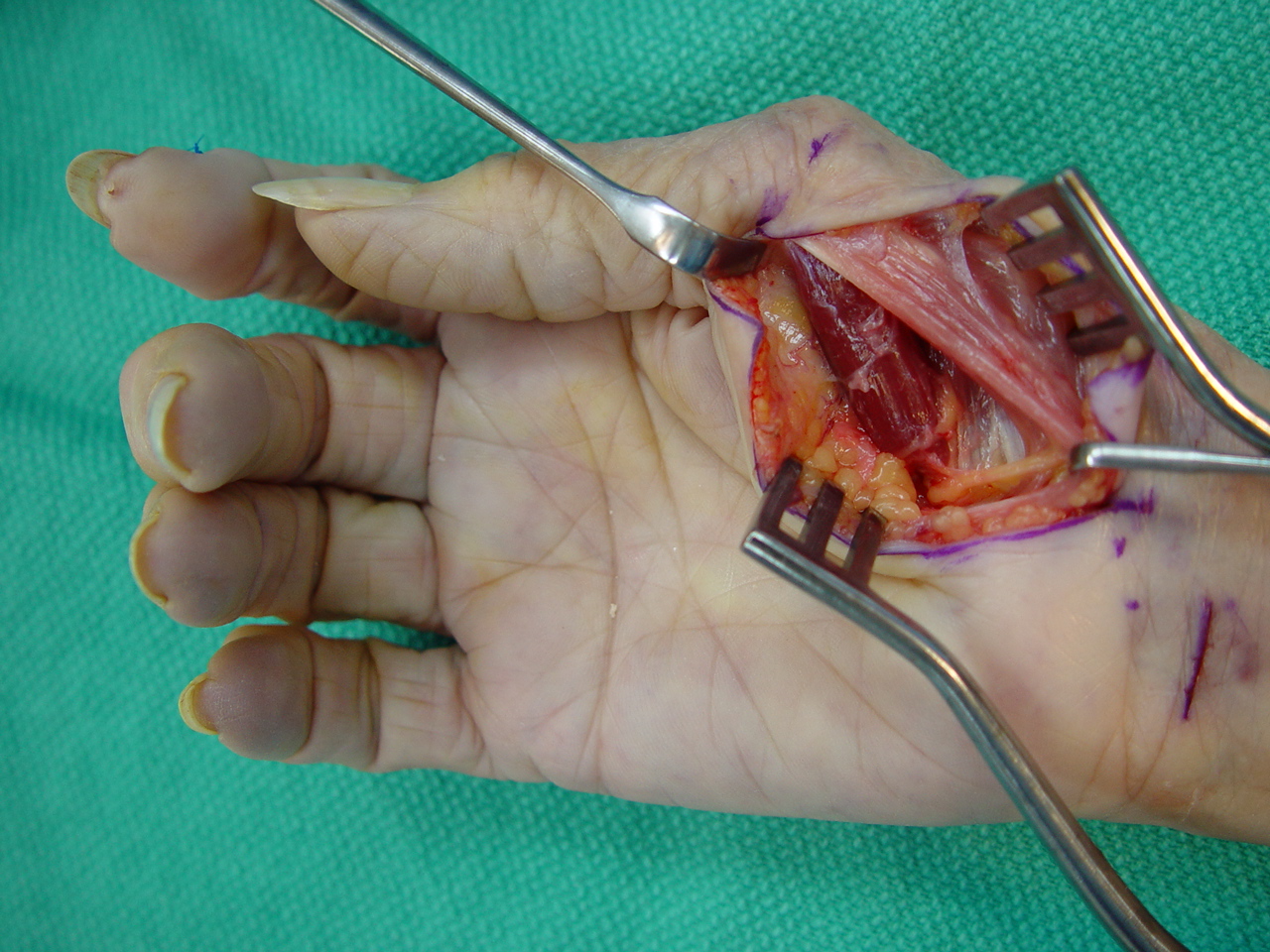
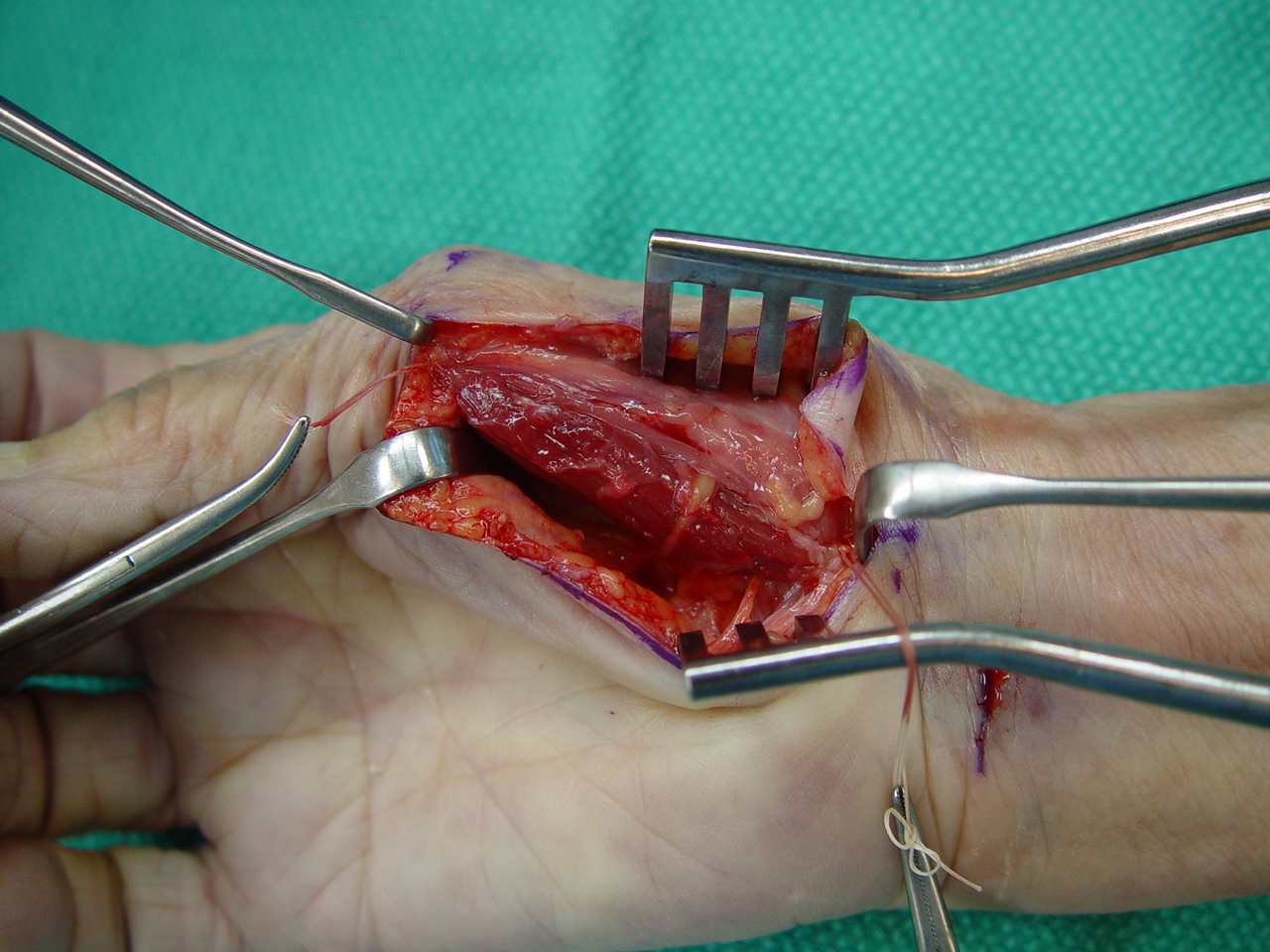
bipolar transfer of the superficial head of the flexor pollicis brevis
to the origin and insertion points of the the abductor pollicis brevis
muscle. The superficial head of the short thumb flexor, with ulnar nerve
innervation, provides thumb opposition in nearly half of patients with
low median nerve palsy. In a smaller percentage of patients with low median
nerve palsy, the short flexor maintains strength but does not provide opposition.
In this group of patients, flexor to abductor transfer may be a satisfactory
alternative, not requiring wrist immobilization and not dependent upon
tenodesis. |